News from practice and research
Important information on endometriosis and related problems such as lower abdominal pain, menstrual cramps and involuntary childlessness are briefly summarized here
Sonographic examination now plays a central role in the diagnosis of endometriosis.
As a result of the efforts of Prof. Dr. J. Keckstein, Dr. med. Sebastian D. Schäfer and Prof. Dr. med. Markus Hoopmann, the AGEM is organizing its first sonography course as an online seminar on 2.9.2023. The event was organized in cooperation with DEGUM, ÖGUM, SGUM, AGE, SEF and EEL.
You can open the program by clicking HERE to view and download the program.
There are still places available – register quickly to secure your place!
#Enzian, the new comprehensive edometriosis classification
As a result of the tireless efforts of Prof. Dr. J. Keckstein and Univ. Doz. Dr. G. Hudelist and other international experts, an endometriosis classification has been developed that combines and optimizes r-ASRM and Enzian. It can be used for non-invasive procedures such as sonography and MRI and, of course, for laparoscopy. It will soon be published in Acta Obstetricia et Gynecologica Scandinavica (AOGS) – probably open access.
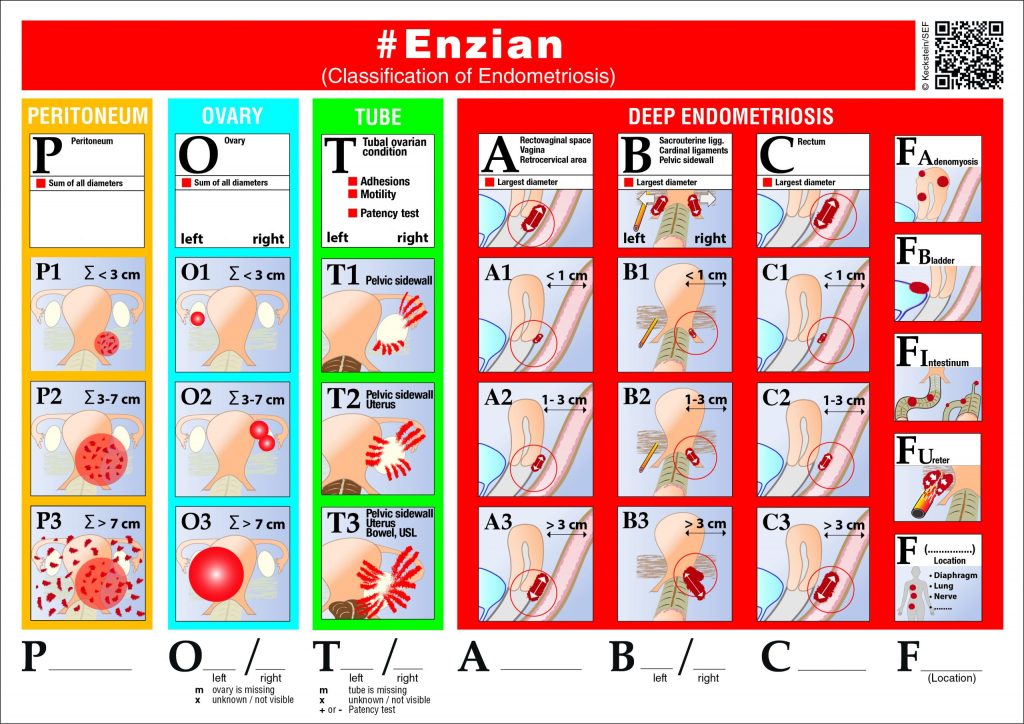
You can download the #Enzian under “Downloads” from the SEF page. With one mouse click HERE you can enlarge the picture.
Webinar to obtain the certificate “Special qualification in the field of endometriosis.”
Due to the corona pandemic, we have implemented the idea of offering the proven 7-hour qualification seminar online as a webinar faster than originally planned. You can register by e-mail(kwschweppe@ewetel.net ) and request activation. Once you have received the access data, you can open the seminar under the “Endometriosis Academy” tab on our website and listen to the lectures online at a time that suits you. You must complete and return the CME questionnaire, which you will also receive after registration. If you have answered more than 75% of the questions correctly – which we are convinced you have – you will receive the certificate issued by the SEF and EEL.
Information on MDNA Life Science’s announcement of a new diagnostic test:
In a press release, MDNA Life Sciences (England) has announced that it has developed a blood test that can diagnose endometriosis in nine out of 10 cases.
- the original work of the company:
https://www.futuremedicine.com/doi/pdfplus/10.2217/bmm-2018-0419 - the statement of the World Endometriosis Society (WES):
http://endometriosis.org/news/research/blood-test-to-diagnose-endometriosis/ - the statement of the SEF:
Endometriosis is really too complex to be detected reliably enough with just one genetic factor in a person’s mitochondria. Conspicuous features: The number of cases in the study is very small; the physicians at the clinic who treated the endometriosis patients are not authors/co-authors of the publication but only employees of the company are listed as authors; the price of the test is high; it is not yet available and it has not yet been validated. Unrealistic hopes may be raised in patients.
The SEF statement was written by Dr. K. Bühler and Prof. Dr. D. Hornung and can be read and downloaded here.
Information about the new homepage:
- All advisory board members must sign the declaration of consent to the use of their data (on the list of advisory board members) in accordance with the GDPR and return it to the SEF secretariat (by post or as a pdf attachment by e-mail).
- Please check the advisory board list to ensure that your details are still up to date, in particular your telephone number and e-mail address. Please send any necessary corrections by e-mail to kwschweppe@ewetel.net.
- Login to the protected member area:
In the dropdown menu “Foundation” last item: Click on “Login”; in the new screen click on “Register” at the bottom and then fill in the fields for the user account. Prof. Schweppe then receives a request and can activate the advisory board member. You then have access with your chosen password. If you have forgotten it, you can now request a new one yourself and not – as in the past – have a new one programmed for money. - You will only find the forum and the member information item in the drop-down menu when you are logged in!
Training:
Prof. Thomas Römer recently held a webinar on the diagnosis and treatment of endometriosis. The approximately one-hour recording is available as a video for continuing education and continuing education points can be earned by answering the CME questions correctly. CME course on endometriosis now available at www.arztcme.de/endometriose-2018.
There is also a CME training course from this year, authored by Prof. Dr. S. Mechsner, which also deals with endometriosis treatment.(https://cme.medlearning.de/jenapharm/therapiekonzepte_endometriose/index.htm)
Selected information on the Weissensee Annual Conference:
- Summary of the complications working group SEF meeting 2018
The following points were discussed at this year’s working meeting as part of the “Complications of TIE surgery” working group:
- Information on the complications of TIE surgery. In this regard, the possibility of fistula formation, anastomotic insufficiency with the need for a stoma, vascular and nerve injuries, bladder emptying disorders, etc. should be pointed out in writing. The addition of “etc.” is recommended in order not to rule out other possible complications.
- Discussion of the possibility of a visitation of endometriosis centers. A list of the centers and the address of the contact person could be published on the SEF website.
- Discussion of the recording of complications of TIE-associated bowel surgery and evaluation of the main surgical technique practiced at the centers (shaving, dissection or segment resection).
- Summary of the Certification Working Group:
Definition of the areas of responsibility of the AG Certification, the Certification Commission and the group of auditors.
- AG Certification:
The Certification Working Group meets regularly on the occasion of the SEF Weissensee Conference; all members of the Certification Commission and all auditors are invited; guests from among the participants of the Weissensee Conference are welcome. The group discusses and develops proposals for changing and optimizing the certification procedure, the certification criteria, etc.. The results are examined by the Certification Commission, modified if necessary and submitted to the SEF Board as a draft resolution. The Board decides on the proposals by simple majority.
- Certification Commission:
For day-to-day business (all receive audit reports and must report back): K.-W. Schweppe, A. D. Ebert, U. Ullrich, M. Beckmann, I. Meinhold-Heerlein and in an advisory capacity: L. Mettler, A. E. Schindler
- Auditors:
The auditors are selected, trained and appointed by EuroEndoCert in agreement with the certification commission. They should be members of the scientific advisory board, they should know the current routine in the clinic or in practice (no longer than 5 years out of active business), they should have attended a course similar to the OnkoZert training course for auditors.
On the occasion of the 8th German Endometriosis Congress in Münster, the following scientific prizes were awarded for the best presentations and posters:
P. Imesch, Zurich
Histone deacetylase inhibitors reduce proliferation in endometriosis cells via epigenetic mechanisms and have an apoptotic effect.
Poster prize Imesch
Histone deacetylase inhibitors reduce proliferation in endometriosis cells via epigenetic mechanisms and have an apoptotic effect
Patrick Imesch
, Michael Schneider, Eleftherios Samartzis, Daniel Fink, André Fedier
University Hospital Zurich, Department of Gynecology, patrick.imesch@usz.ch
The pathogenesis of endometriosis is still not fully understood. Numerous hypotheses and models have been formulated, but many questions remain unanswered. Epigenetic changes such as acetylation of histones are increasingly being discussed as a possible pathomechanism of endometriosis. Histone deacetylase inhibitors (HDACi) are a class of substances that can alter the gene expression pattern by changing the chromatin structure and thus have an epigenetic regulatory effect. It is assumed that 2-5% of the genome can be influenced by HDACi. Interestingly, these are often genes that are involved in proliferation and apoptosis control.
The aim of the work was to find out whether endometriosis cells are in principle target cells for the HDACi romidepsin and whether this has an effect on the proliferation rate and apoptosis behavior. The investigations were carried out using standard cell biology and molecular biology methods (Western blot, RT-PCR, MTT) on an immortalized epithelial endometriosis cell line.
The basic proof of efficacy of romidepsin was clearly demonstrated by the reduction of total histone deacetylase activity on the one hand and by the accumulation of acetylated histones on the other. This resulted in an upregulation of the cell cycle inhibitor p21 and a downregulation of cyclins B1 and D1, which also led to a significant inhibition of proliferation. At higher doses (from 20nM), an activation of the intrinsic apoptosis pathway was also detected. In further studies, some genes important in the pathomechanism were examined with regard to regulation. It could be shown that in subapoptotic doses of romidepsin, a downregulation of the proangiogenic factor VEGF and of the matrix-degrading enzymes MMP-2 and -9 could be achieved. At the same time, E-cadherin, an adhesion molecule with invasion suppressor properties, could be upregulated. The resulting reduced migratory potential was demonstrated in simple wound-healing assays.
The studies show that endometriosis cells are indeed target cells for HDACi and that the regulation of relevant genes can be influenced as a result. HDACi thus represent a new, promising, epigenetically active therapeutic option for the treatment of endometriosis. The results also support the possible importance of epigenetics in the pathogenesis of endometriosis.
- Agic, Lübeck
Inhibition of cell proliferation, adhesion and invasion with monoclonal antibodies against L1 cell adhesion molecule (L1CAM) in an in vitro endometriosis model.
Poster price Agic
Inhibition of cell proliferation, adhesion and invasion with monoclonal antibody against L1 cell adhesion molecule (L1CAM) in an in vitro endometriosis model
Agic A.1, Diedrich K.1, Altevogt P.2, Starzinski-Powitz A.3, Hornung D.1
1
University of Lübeck, Women’s Clinic, Lübeck, Germany,
2DKFZ, Tumor Immunology Program, Heidelberg, Germany,
3JohannWolfgang Goethe University in Frankfurt am Main, Human Genetics, Frankfurt am Main, Germany
Endometriosis is a benign and usually progressive disease. The cell adhesion molecule L1CAM is overexpressed in ovarian and endometrial cancer and is associated with a poor prognosis. Our previous studies showed increased L1 expression in endometriosis, which prompted us to investigate L1-mediated proliferation, adhesion and invasion in an in vitro endometriosis model. Cell proliferation and survivability were investigated in a proliferation assay using an endometriosis cell line Z12. L1-mediated adhesion and invasion and their inhibition by anti-L1 antibodies were also investigated with the endometriosis cell line Z12 in the so-called “sandwich assay” using Matrigel®. The proliferation of endometrial epithelial cells Z12 decreased significantly after preincubation with monoclonal anti-L1 antibody (10µg/ml) (P< 0.001, 0.95 ± 0.34 x 300,000 cells) compared to preincubation with unspecific IgG-mAb (3.88 ± 1.16 x 300,000 cells) and to untreated cells (3.63 ± 1.12 x 300,000 cells). The relative invasion of Z12 cells through Matrigel® was significantly inhibited (P< 0.001) after preincubation with monoclonal anti-L1 antibody (26.40 ± 13.50 %) compared to preincubation with non-specific IgG-mAb (76.04 ± 24.06 %) and untreated cells (76.30 ± 26.84 %). Monoclonal anti-L1 antibody was also able to inhibit Z12 cell adhesion (P< 0.001, 68.69 ± 16.71 %) compared to non-specific IgG-mAb (89.49 ± 23.78 %) and untreated cells (90.00 ± 21.53 %). Based on our results, we assume that L1 favors the development of endometriosis by increasing cell invasion and adhesion and worsens the prognosis. In further studies, the monoclonal L1 antibody will be tested in an endometriosis animal model.
Wolf, M.*, Schüring, A.N.*, Schulte, N.*, Staebler, A.+, Kiesel, L.*, Buchweitz, O.*, Götte, M.*
(* Frauenklinik Münster, + Inst. f. Pathologie Tübingen)
Altered expression of the pluripotency-associated transcription factor Sox2 in endometriosis.
Wolf poster prize
Altered expression of the pluripotency-associated transcription factor Sox2 in endometriosis
Wolf, M.1, Schüring A.1, Schulte N.1, Staebler A.2, Kiesel L.1, Buchweitz
O., Götte M.1
1Clinic and Polyclinic for Gynecology and Obstetrics, University Hospital Münster, Albert-Schweitzer-Str. 33, D-48149 Münster; 2Instituteof Pathology; University Hospital Tübingen; Contact: Maria_Wolf@email.de; mgotte@uni-muenster.de
Cyclical processes of regeneration, cell differentiation and desquamation take place in the human endometrium during the menstrual cycle. The basis of this high regenerative capacity is assumed to be the involvement of stem cells. The involvement of endometrial stem cells in the pathogenesis of endometriosis and endometrial carcinoma is also being discussed. Since endometrial stem cell populations are poorly characterized, there is a need to identify molecular markers of endometrial progenitor cells. One possible candidate is the transcription factor Sox2.
This is essential for maintaining the self-renewal potential in undifferentiated embryonic stem cells and is one of the key factors for the production of induced pluripotent stem cells. In this study, the expression of Sox2 in the human endometrium was characterized in order to investigate a possible stem cell involvement in the pathogenesis of endometriosis.
Conventional immunohistochemistry, quantitative real-time PCR (qPCR) and double immunofluorescence studies of physiological and pathologically altered endometrial biopsies (n = 49 patients) were used to comparatively characterize Sox2 expression.
Quantitative rt-PCR was used to detect the expression of Sox2 in the endo- and myometrium. A partial co-expression of Sox2 and telomerase was detected by immunofluorescence microscopy. Using immunohistochemical staining, Sox2-positive single cells and cell groups were identified in the endometrial stroma, as well as single cells in glands and diffuse glandular staining. Quantification using standardized visual field analysis showed a significant increase in Sox2 expression by a factor of 2.1 in proliferative vs. secretory tissue. In contrast, the number of Sox2-expressing stromal cells/facial field was significantly reduced by a factor of 0.50 in endometrial cancer tissue compared to proliferative endometrium. Sox2 expression in endometriosis biopsies was ambivalent. The number of Sox2-positive cells was significantly increased in the stroma compared to the secretory tissue, while the Sox2-positive glands were significantly reduced by 70% compared to endometrial carcinoma.
The high proliferative and pluripotent potential of Sox2-positive cells could lead to cells that have entered the abdominal cavity during retrograde menstruation adhering, implanting and manifesting endometroid lesions. The reduced expression of the transcription factor Sox2 in endometrial carcinoma corresponds to current studies on the function of Sox2 as a tumor suppressor gene in gastric carcinogenesis. Further histopathological studies on larger patient collectives to analyze the prognostic value of the Sox2 marker appear worthwhile in order to demonstrate its clinical relevance for the pathogenesis of endometriosis.